 Post Reply
6521-6540 of 10899
Post Reply
6521-6540 of 10899
Hi!Millioaire!!!!!!!!!!!!
How to make money? Bought at $0.69
Bought at $0.69

jackjames ( Date: 25-Jun-2008 09:26) Posted:
oh please, this is not for A-level biology class or medicine courses la..
just tell us when is the takeover date, and the bid price to merge the company... that's it.... we are interested in $$$$$ !!! ha ha.. |
|
I am not "Tua Peh Kong" lah..so cannot tell you when takeover date and bid price... I am just human.. so can only give factual information..  Ha ha..
Ha ha..
jackjames ( Date: 25-Jun-2008 09:26) Posted:
oh please, this is not for A-level biology class or medicine courses la..
just tell us when is the takeover date, and the bid price to merge the company... that's it.... we are interested in $$$$$ !!! ha ha.. |
|
Thanks P-A-E, explanations and illustrations clear as crystal...couldn't ask for more. Info provided by you and Bengster and a few others are so detailed that help me decide whether or not to INVEST in Biosensors .
oh please, this is not for A-level biology class or medicine courses la..
just tell us when is the takeover date, and the bid price to merge the company... that's it.... we are interested in $$$$$ !!! ha ha..
Hi PensionAlterEgo,
Thank you for making the effort to post the information for all. It will definitely help us to appreciate the issue more.
I now have more confident on BIG. With such low price now, I regreted for 'firing' all my bullets during the early days of mkt down trend. I should have preserve my ammo for the great 'killing' !
Oh my... Too much to digest. In summary...?
Part 2
Intimal hyperplasia
Hyperplasia is a general term referring to the proliferation of cells within an organ or tissue [7]. Hyperplasia may result in the gross enlargement of an organ or the formation of a benign tumor.
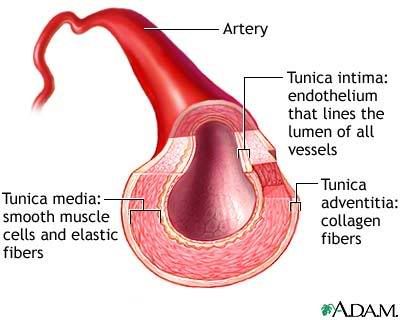 Figure 4. Arterial wall. Image taken from [1].
Figure 4 shows the make up of the arterial wall. The Tunica Intima (or just Intima) is the innermost layer of an artery. It is made up of one layer of endothelial cells (cells to reduce friction between artery wall and blood) and is supported by an internal elastic lamina. The endothelial cells are in direct contact with the blood flow. Intimal hyperplasia is started by damage to the vascular wall during angioplasty and may, in fact, be exacerbated by the metal stents [6]. Damage to the vascular wall results in endothelial erosion, triggering a process of thrombosis (blood clot) and leading to smooth muscle cell migration and proliferation at the site of injury. Immune cells also infiltrate into the site of the wound and promotes cell proliferation. Neointimal proliferation (access growth) is positively associated with deeper medial penetration of stent struts (see Figure 4) [6]. The deeper the stent cuts into the Tunica Intima and Tunica Media, the worse it is. Medial disruption and plaque fracture by stent struts is associated with greater numbers of inflammatory cells.
Measuring restenosis
There are many parameters that are used to measure or gauge the efficacy of a drug eluting stent with regards to restenosis. In some trial results, we often see a term known as Angiographic binary restenosis (ABR). It is basically the percentage of patients with a follow-up percent diameter stenosis of greater or equal to 50% determined by quantitative coronary angioplasty. Figure 5 explains the blockage clearer.
Figure 4. Arterial wall. Image taken from [1].
Figure 4 shows the make up of the arterial wall. The Tunica Intima (or just Intima) is the innermost layer of an artery. It is made up of one layer of endothelial cells (cells to reduce friction between artery wall and blood) and is supported by an internal elastic lamina. The endothelial cells are in direct contact with the blood flow. Intimal hyperplasia is started by damage to the vascular wall during angioplasty and may, in fact, be exacerbated by the metal stents [6]. Damage to the vascular wall results in endothelial erosion, triggering a process of thrombosis (blood clot) and leading to smooth muscle cell migration and proliferation at the site of injury. Immune cells also infiltrate into the site of the wound and promotes cell proliferation. Neointimal proliferation (access growth) is positively associated with deeper medial penetration of stent struts (see Figure 4) [6]. The deeper the stent cuts into the Tunica Intima and Tunica Media, the worse it is. Medial disruption and plaque fracture by stent struts is associated with greater numbers of inflammatory cells.
Measuring restenosis
There are many parameters that are used to measure or gauge the efficacy of a drug eluting stent with regards to restenosis. In some trial results, we often see a term known as Angiographic binary restenosis (ABR). It is basically the percentage of patients with a follow-up percent diameter stenosis of greater or equal to 50% determined by quantitative coronary angioplasty. Figure 5 explains the blockage clearer.
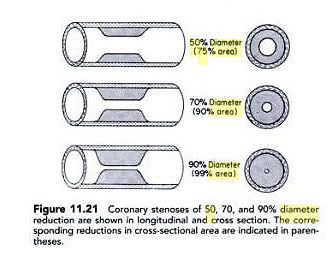 Figure 5. Coronary Stenosis. Image taken from [8]
In the first artery, the blockage is 50% in diameter or it simply means that 75% of the lumen (blood flow) area is blocked. When this happens a patient will contribute to the binary restenosis score in the DES trials. A severe case of restenosis or severe late lumen loss would lead to the need for revascularization.
Revascularization is the process of restoring the functionality of an affected organ; in this case the artery. We often see another term TLR, used in DES clinical trials. Target lesion revascularization (TLR) is defined as any repeat revascularization procedure (percutaneous or surgical) of the original target lesion site, which includes the stented plus edge (typically 5 mm away from each side of the stent) segments [4]. My interpretation of percutaneous is the repeat process of balloon angioplasty within the previously stented area. Surgical revascularization is basically a Coronary artery bypass graft (CABG). I am not sure if a repeat procedure of stenting over the old lesion is normally done and considered as revascularization. At the moment, I cannot find any document to support this fact.
Another often seen measurement of restenosis is late lumen loss. But this is not the best surrogate (substitute) endpoint for restenosis. Late lumen loss as a surrogate (substitute) endpoint for restenosis is used in DES trials because it significantly reduces the number of patients that need to be recruited [9]. Note that target lesion revascularization TLR is the most relevant endpoint to physicians and most importantly, to patients. Physicians are primarily concerned with whether the patients are going to come back with recurrent symptoms. By definition, TLR is what ultimately brings the patient back and not the measure of lumen loss [9]. This makes sense since lumen loss only given an indication how much growth has occurred. It has a weak correlation to TLR and is sometimes use to predict the number of revascularization that needs to be done. Therefore, clinical outcome, particularly target lesion revascularization (TLR), is regarded as the true measure of success for anti-restenosis therapies [9].
The following section provides a glossary of terms that are often found in DES clinical trial reports.
Figure 5. Coronary Stenosis. Image taken from [8]
In the first artery, the blockage is 50% in diameter or it simply means that 75% of the lumen (blood flow) area is blocked. When this happens a patient will contribute to the binary restenosis score in the DES trials. A severe case of restenosis or severe late lumen loss would lead to the need for revascularization.
Revascularization is the process of restoring the functionality of an affected organ; in this case the artery. We often see another term TLR, used in DES clinical trials. Target lesion revascularization (TLR) is defined as any repeat revascularization procedure (percutaneous or surgical) of the original target lesion site, which includes the stented plus edge (typically 5 mm away from each side of the stent) segments [4]. My interpretation of percutaneous is the repeat process of balloon angioplasty within the previously stented area. Surgical revascularization is basically a Coronary artery bypass graft (CABG). I am not sure if a repeat procedure of stenting over the old lesion is normally done and considered as revascularization. At the moment, I cannot find any document to support this fact.
Another often seen measurement of restenosis is late lumen loss. But this is not the best surrogate (substitute) endpoint for restenosis. Late lumen loss as a surrogate (substitute) endpoint for restenosis is used in DES trials because it significantly reduces the number of patients that need to be recruited [9]. Note that target lesion revascularization TLR is the most relevant endpoint to physicians and most importantly, to patients. Physicians are primarily concerned with whether the patients are going to come back with recurrent symptoms. By definition, TLR is what ultimately brings the patient back and not the measure of lumen loss [9]. This makes sense since lumen loss only given an indication how much growth has occurred. It has a weak correlation to TLR and is sometimes use to predict the number of revascularization that needs to be done. Therefore, clinical outcome, particularly target lesion revascularization (TLR), is regarded as the true measure of success for anti-restenosis therapies [9].
The following section provides a glossary of terms that are often found in DES clinical trial reports.
Glossary of vascular terms [10]
Angiographic binary restenosis (ABR)Percentage of patients with a follow-up percent diameter stenosis of greater or equal to 50%. See Figure 5 above.
AngioplastyA procedure used to unblock an artery clogged with plaque; also known as percutaneous transluminal coronary angioplasty (PTCA), or balloon angioplasty.
Coronary arteryAn artery of the heart that supplies oxygenated blood.
Coronary artery bypass graft (CABG)An invasive medical procedure in which a section of an artery from another portion of the body is used to bypass a blockage in a coronary artery to improve blood flow to the heart.
De novoNew, untreated; In trial reports, de novo simply means a coronary artery that has not been previously treated.
Dual antiplatelet therapyThe combination of aspirin and a second anticlotting medication such as clopidogrel (also called Plavix®) to reduce the risk of blood clots following stent implantation.
EndothelializationFollowing stent implantation, the healing process of tissue regrowth over the stent to prevent thrombosis.
In-segmentA measurement of the length of a deployed stent plus 5 millimeters on either side of the stent.
In-stentA measurement of the length of the deployed stent.
Late lossThe difference in measurements of a blood vessel lumen diameter before and after a stent procedure, as shown with angiography.
Late stent thrombosisA blood clot that forms on the stent 30 days to 1 year post-implant.
LesionA blockage in a blood vessel that is interrupting blood flow to the heart, often due to plaque
LumenThe cavity or hollow space inside a blood vessel.
Major adverse cardiac events (MACE)Clinical events following a stent procedure that include death, myocardial infarction (heart attack), emergent CABG (bypass) and target lesion revascularization. Note that as long as any of these 4 clinical events appear, it contributes to the MACE rate/numbers.
Neointimal hyperplasiaA medical term indicating the abnormal growth of new tissue over a stent.
Percutaneous coronary intervention (PCI)A minimally invasive procedure to treat narrowed arteries. Commonly known as coronary angioplasty or simply angioplasty. The term balloon angioplasty is commonly used to describe percutaneous coronary intervention, which describes the inflation of a balloon within the coronary artery to crush the plaque into the walls of the artery.
RestenosisThe renarrowing of an artery in the same location of a previous treatment; clinical restenosis is the manifestation of an ischemic event, usually in the form of recurrent angina (heart attack).
RevascularizationA procedure to unblock or bypass a clogged artery. My interpretation is that plain balloon angioplasty is probably one of the revascularization methods used over the previously stented area. Bypass is another method. Note that, I am not sure if re-stenting over the old stent is normally done. At the moment, I am not able to say if this is a revascularization method.
Stent thrombosisA blood clot that forms on the stent; categorized as early stent thrombosis (030 days post-implant), late stent thrombosis (30 days 1 year post-implant) and very late stent thrombosis (more than 1 year post-implant).
Target lesion revascularization (TLR)Any repeat percutaneous intervention of the target lesion or bypass surgery of the target lesion. Note that this includes balloon angioplasty and bypass done over the old lesion. TLR is a very important measurement for DES trials.
Target vessel failure (TVF)When a patient experiences death, myocardial infarction (heart attack), emergent CABG, revascularization in the target lesion (TLR) or revascularization in the target vessel, which was previously stented, then this event contributes to the TVF value. TVF is basically the combination of 4 events of MACE plus the single event of TVR. If the 5 events above happen due to another vessel, it does not contribute to the TVF value.
Target vessel revascularization (TVR)Revascularization needed when a patient experiences a recurrence of symptoms and the lesion is somewhere along the length of the previous vessel treated. Note that this is a measure of revascularization in the same vessel but not in the previously stented segment. If revascularization happens on the previous lesion, this is TLR.
ThrombosisThe formation of blood clots in arteries that can lead to myocardial infarction or death.
Very late stent thrombosisA blood clot that forms on the stent 1 year or more post-implant.
References
[1] http://www.nhlbi.nih.gov
[2] http://carefirst.staywellsolutionsonline.com/
[3] http://en.wikipedia.org/wiki/Stenosis
[4] www.cathlabdigest.com/article/5422
[5] Americal Journal of Medicine, 2003; 115: 547-553
[6] Coolong A, Kuntz RE, Understanding the drug-eluting stent trials, Am J Cardiol. 2007 Sep 3;100(5A):17K-24K. Epub 2007 Jun 26
[7] http://en.wikipedia.org/wiki/Hyperplasia
[8] Donald S. Baim, William Grossman, Cardiac Catheterization, Angiography, and Intervention, 2005 - Medical - 807 pages
[9] www.theheart.org/documents/docs34000/34437/Late_Loss_TLR.pdf
[10] wwwp.medtronic.com/newsroom/content/1199737441831.pdf
Hi all, the following is a document that I tried to put together so that fellow forumers will be able to understand some of these mind boggling terms that we often see in clinical trial reports. With this, I hope that more forumers will be able to understand and appreciate the superiority of BIG's Biomatrix stents. Thanks to bengster for providing some initial comments and suggestions for changes. I am not sure if this forum allows me to post a long document.. so I am going to split into several parts.
Part 1.
Disclaimer:
I am not medically trained and the information provided in this document is not a medical advice. The concepts and points collected herein could have been misinterpreted by me. Readers are encouraged to obtain the help, services and recommendations of doctors and other licensed medical practitioners. The purpose of this document is to facilitate dissemination of information about how to interpret drug eluting stent trial results. The images, text and contents contained in this document are for informational purposes only and not intended to substitute for the medical advice of a qualified physician, therapist or other trained professional. The contents of this document have been mostly borrowed from many different sources.
Stenting Process
Figure 1. Stenting process. Image borrowed from [1].
Figure 1 describes the stenting process in the coronary artery with plaque buildup [1]. Plaque is made up of fat, cholesterol, calcium, and other substances found in the blood [2]. The coronary artery is located on the surface of the heart. Figure 1A shows the deflated balloon catheter (also a process of angioplasty) and closed stent inserted into the narrowed coronary artery. The insert image on figure 1A shows a cross-section of the artery with the inserted balloon catheter and closed stent. In figure 1B, the balloon is inflated, expanding the stent and compressing the plaque to restore the size of the artery. Figure 1C shows normal blood flow restored in the stent-widened artery. The insert image on figure 1C shows a cross-section of the compressed plaque and stent-widened artery. When the plaque is compressed and the stent is expanded, the walls of the artery will naturally get damaged.
Restenosis
A common problem after angioplasty is too much tissue growth within the treated portion of the artery. This can cause the artery to narrow or close again, which is called restenosis. This problem is often avoided with the use of newer stents coated with medicines that help prevent too much tissue growth [1].
Figure 2. Restenosis of a Stent-Widened Coronary Artery. Image from [1]
The illustration in Figure 2 shows the restenosis of a stent-widened coronary artery. The coronary artery is located on the surface of the heart. In figure 2A, the expanded stent compresses plaque, allowing normal blood flow. The inset image on figure 2A shows a cross-section of the compressed plaque and stent-widened artery. In figure 2B, over time, the plaque grows through and around the stent, causing a partial blockage and abnormal blood flow. The inset image on figure 2B shows a cross-section of the growth of the plaque around the stent. Note that in this example, the plaque is shown as the cause of the re-narrowing or stenosis (abnormal narrowing in a blood vessel [3]). Stenosis can be caused by other means as well. An important one is the inflammatory response, which induces tissue proliferation around an angioplasty site (see Neointima Proliferation or Intimal Hyperplasia below) [3]. An analogy for this is some scarring on your skin that might sometime protrude out when you get a deep cut. In Figure 2B, the restenosis occurring inside the stent section is termed as in-stent restenosis. The restenosis inside plus 5 mm just outside the stent on both sides of the stent is known as in-segment restenosis.
Mechanism of In-Stent Restenosis
The mechanism/manifestation of restenosis can be explained by the lumen loss due to the process of angioplasty. Lumen loss is the difference in millimeters between the diameter of a stented segment post-procedure and at any time of interest [4]. Or putting it in simple terms, mean the loss of the blood vessel flow area due to the in-growth. Note that in most trials, late lumen loss is tabulated to give an idea of how much growth has occurred (thickness in millimeter). Figure 3 shows the artery cross section over a period of time when stenting (stent + balloon angioplasty) and plain balloon angioplasty is done.
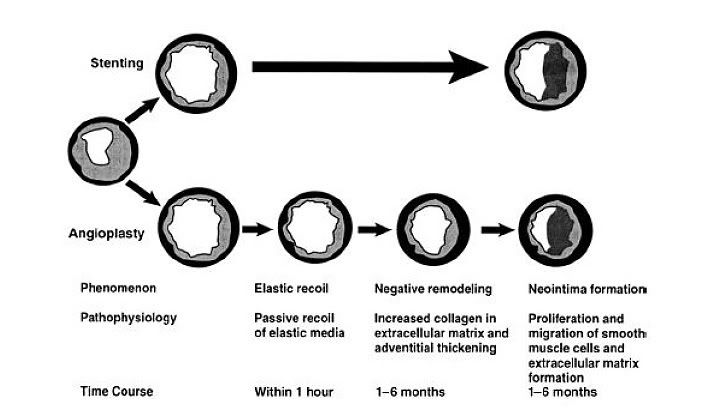
Figure 3. Lumen losses. Image taken from [5]
From Figure 3 above, when balloon angioplasty is carried out, early lumen loss (within 1 hour of the procedure) is attributed to elastic recoil. This of course is not present in the stenting process because the stent acts as a scaffolding to prevent the recoil. Stents also reduces the impact of negative remodeling on lumen area when compared to plain balloon angioplasty [6].
Two mechanisms contribute to late lumen loss in patients undergoing Angioplasty are negative remodeling and intimal hyperplasia (indicated as Neointima formation in Figure 3). Note that in this example, the intimal hyperplasia is due to abnormal tissue growth and not plaque. Intimal hyperplasia remains a problem in stenting as well as plain balloon angioplasty.
Good price, tempted to acc but low vol leh, lack of support power, moreover alrdy holding some leow. observe further loh.
BIG also has a BiolimusA9 ABSORB fully bioabsorbable DES using 100% PLA biodegradable polymer. So this technology is not new. Abbott also has their Everolimus ABSORB DES as well. Many people are already ahead of Freedy Boey. If BIG had their CE mark in 2006, BIG would have the cash to intensify R&D and clinical trial for their own BiolimusA9 ABSORB DES and perhaps can obtain its CE Mark in 2009. Abbott is expected to obtained their ABSORB DES CE approval somewhere in 2009 or 2010. I feel this absorb/soluble DES technology is rather "questionable" and may not work well.
Hi Bengster,
Thanks for the insights. Actually, was never worried about the funds Prof Freddy Boey is getting. Rather, its seems that this soluble stent business is generating much interest not only by the commercial but also the state. Why else would they throw $10m into the research if there is no value??
To me, all the more it seems that BIG is moving in the right direction. The more interest (positive of course) generated, the better and easier for BIG to promote their products.
***Victory89: Firstly, congrats to Prof Freddy Boey for getting the NRF funds..
Actually, I kind of know his story a little bit. He tried to sell his stent invention to a few companies (travelled to a Europe & US etc.. ) but there were no takers.. but eventually got Bio One (EDB linked) to pump in money to start up Amaranth Medical.
I have seen Freddy Boey's presentation before.. Looks impressive but very very far from commecialization. What do you expect.. he is a Materials guy.. not a MD or a biomed.
Has patents filed for stents, the earliest in 2005 but not granted yet.. and it mostly covers the stent design (mostly materials aspects). So has a long way to learn the ropes.. about true DES designs.
Last trial done on animals was around 2006. Since 2006, there was talk about human trials. Up till now, no human trials yet..
So make your own conclusion about this news..
***Bengster: There are many wild claims of revolutionary DES that has potential but until these companies can come out with a solid set of human clinical trial reports, all are baseless claims. This stent will take at least 5 more years to get commercialisation approval.
If Prof Freddy Boey is just a "Materials Engineer", then he has a lot more to learn about making a good DES. The stent design engineering, biomed knowledge, pharmaceutical knowledge, chemical knowledge and many other fields of knowledge are required and carefully formulated to make a good DES. This company now only has an "Angel" investor Bio One (EDB). Remeber the strongest point of a DES is the weakest link that is holding all the complicated DES composition parts together. One single weak area can cause the whole stent program to fail even if they score full marks for the rest of the composition parts. This new stent foetus has not even past its first-trimester pregnancy.
Centaur ( Date: 24-Jun-2008 15:35) Posted:
Sorry Not sure if it came out. Repost as below.
Research on soluble heart stents get $10m boost
A NANYANG Technological University (NTU) professor hopes to be testing soluble stents on heart patients here within two years.
Professor Freddy Boey just got a $10 million leg-up for his work.
His is among four promising research teams here which have been awarded up to $10 million apiece over three to five years by the National Research Foundation (NRF).
Three of the teams are from NTU, and the fourth, from the National University of Singapore.
Prof Boey, who has been working on the stent for five years , said: 'This award is recognition of the work we do.'
Stents used now are tiny metal wire-mesh tubes, sometimes coated with drugs, which are inserted into the blood vessels to keep them open and the blood flowing, to prevent a heart attack.
The one he and his team are developing is considered the holy grail of stents because it dissolves completely over time and releases drugs or proteins to prevent side-effects such as blood clots. Because no foreign body remains in the vessel, it can heal faster, cutting the risk of it becoming clogged over the next few years. |
|
Sorry Not sure if it came out. Repost as below.
Research on soluble heart stents get $10m boost
A NANYANG Technological University (NTU) professor hopes to be testing soluble stents on heart patients here within two years.
Professor Freddy Boey just got a $10 million leg-up for his work.
His is among four promising research teams here which have been awarded up to $10 million apiece over three to five years by the National Research Foundation (NRF).
Three of the teams are from NTU, and the fourth, from the National University of Singapore.
Prof Boey, who has been working on the stent for five years , said: 'This award is recognition of the work we do.'
Stents used now are tiny metal wire-mesh tubes, sometimes coated with drugs, which are inserted into the blood vessels to keep them open and the blood flowing, to prevent a heart attack.
The one he and his team are developing is considered the holy grail of stents because it dissolves completely over time and releases drugs or proteins to prevent side-effects such as blood clots. Because no foreign body remains in the vessel, it can heal faster, cutting the risk of it becoming clogged over the next few years.
30/05/08 OCBC Research
Leaner, Meaner and Better
BioMatrix sales and clinical interest.
of US$1.7m from its BioMatrix DES in 4QFY08 after it sold some "prelaunch"
units during the quarter. Though sales is currently insignificant,
clinical interests displayed at the recent EURO PCR conference in May
08 was described as "overwhelming" where attendance at its symposium
was reduced to standing room. We view this intense interest in Biosensor's
technology at such key clinical events as a harbinger of healthy sales of
BioMatrix.
Biosensors booked maiden sales
Tectonic operational restructuring
operations and cut redundancy, Biosensors will be closing down its Newport
Beach manufacturing facility in the US and has plans to divest or cease
operations in Occam located in Netherlands (currently producing older
Axxion stent model). All of its manufacturing functions will be shifted to
Singapore to capitalise on its lower cost base. However, Biosensors will
retain its R&D function and a corporate office in the US. Management has
indicated that the reduction in operational expenses of US$7-9m/year will
be ploughed back into R&D.
. In a bold move to streamline
Critical China piece.
Weigao remains a crucial piece in Biosensor's earnings forecast of US$100-
115m for FY09 and beyond. Management has assured us that it is in both
party's interest for the sale to go through as Biosensors would be able
better able to bring JWM into its next phase of growth with technology
transfers.
The full acquisition of JW Medical from Shandong
Turnaround story
contribution from JWM, restructuring to cut redundancies, good
management in place and lower cost based productions in Singapore and
China, we urge investors to view their investment options in Biosensors
with a longer term horizon.
. With a massive ramp up in BioMatrix sales, positive
Ruminating valuations
strategic roadmap and has executed its plans well so far. Also, in a strong
show to ensure good operational execution, Biosensor's CEO will now be
based out of Singapore. We use a standard medtech valuation methodology
by discounting its first year of substantial profit in FY10 to present day
value. Our fair value stands at S$1.04. Maintain
Section 1: FY08 results overview
Improved results.
in revenue to US$44.3m as product sales rose 14% and it started to reap
licensing revenue. It remained in a loss-making position but that narrowed
17% to -US$30m. Average product gross margin came in slightly lower at
39% (vs. 41% in FY07) due to delays in moving operations to China and
inventory write-offs. The results were in line with our expectations.
For its FY08 results, Biosensors reported a 29% increase
Iteration of guidance.
revenue in FY09. The revenue guidance is dependent on the full acquisition
of JW Medical (JWM) in China. On a stand alone basis, Biosensors is
expecting to make US$65-75m in FY09 revenue, almost a doubling of its
FY08 performance. Pushing the guidance envelope further out to three
years, Biosensors is expecting revenue of about US$250m in FY11.
Management has guided for US$100-115m of
Getting into the black.
return to the black in 4QFY09, we take a more conservative stance and
assume a return to the black in 1QFY10. Our stance is based on inherent
risks of execution in this critical year of transformation from being a solely
technology oriented company into an efficient manufacturer of stents. Again,
assumptions are contingent the full acquisition of JWM.
Although management is guiding that it would
One-time charges in 1Q FY09.
of one-time charges in relation to streamlining its operations in New Port
Beach, USA and Eindhoven, Netherlands. 4QFY08 incurred a charge of
US$3.7m for write down of inventories in its Netherlands Occam facility
while 1QFY09 will record another US$3-4m in restructuring charges. Overall,
the consolidation will reap about US$7-9m/year in operational savings and
this is expected to be ploughed back into R&D.
Section 2: Leaner strategic roadmap
BioMatrix sales and clinical interest.
of US$1.7m from its BioMatrix DES after it sold some pre-launch units
during 4QFY08. Though sales is currently insignificant, clinical interests
displayed at the recent EURO PCR conference in May 08 was described
as overwhelming where attendance at its symposium was reduced to
standing room. We view this intense interest in Biosensors technology at
such key clinical events as a harbinger of healthy sales of BioMatrix.
Biosensors booked maiden sales
Leaner and better.
Investigational Device Exemption (IDE) procedures. As such, Biosensors
will take a strategic step back from its aggressive penetration into the US
and focus its energies on the markets in the EU and Asia. In three years,
the company is targeting a 10% market share in the EU (about US$160m)
and 30% market share in China (about US$120m). Assuming the DES
market grows annually at a very conservative 20% from its current size of
US$1.6b in the EU and US$0.4b in China, the total addressable market
share in these 2 geographies would be about US$2.4b. If executed as
guided, this could translate to a possible topline of US$483m in FY11 for
these two markets alone.
The US FDA has revealed new refinements on its
Not out of US completely.
fulfil its regulatory filing obligations to its licensees Devax and Xtent.
Biosensors will still retain its presence in La Jolla, USA, which is a hotbed
for technology innovation, to evaluate its technology, product and regulatory
positions. We do not rule out Biosensors partnering other companies to
bundle technologies/products for a more holistic offering and a more
defensible position.
Section 3: News flow from major medical conferences
Competing with hard core data.
understands that the bigger, better branded and more well-capitalised
competitors in the market will come out with all cylinders firing to quell any
competition. Thus, we think that it has taken the right path to competing in
this space with well designed and statistically significant clinical trials.
We think that Biosensors fully
Continuous proof.
from the industry thus far, Biosensors is not sitting on its laurels and has
embarked on registries in Asia (BEACON II, 1000 patients) and in the EU
(E-BIOMATRIX, 5000 patients) that started recruitment in Mar 08. Unlike
clinical trials, registries are not designed to fare against another competing
product but involve paying patients who are willing to be tracked over a
certain period of time. We think that its embarkation on such extensive
registries in two different markets is a display of a strong show of confidence
in the long term outcome of its BioMatrix DES.
Despite obtaining data that heralded positive comments
LEADERS trial.
against J&Js sirolimus eluting Cypher DES, to be presented at key clinical
conferences like ESC (Aug 08) or TCT (Oct 08). Although no indications on
the results have been announced, we got positive vibes from management.
This news flow may be a positive stock price catalyst
Section 4: Alliances
Terumo
A tricky piece.
the view that Biosensors relationship with Terumo will be one of the key
factors in the magnitude of its earnings acceleration. The conundrum now
is that Terumo has a non-exclusive distribution right (excluding Japan and
the US) to sell its NOBORI DES (uses Biosensors technology) where
Biosensors is also pursuing sales of its BioMatrix DES in the same region.
Terumo has a wider marketing footprint while Biosensors is limited in this
aspect but may make up for it via the depth of its relationships with clinicians.
Other than its full acquisition of JWM, we continue to hold
Think win-win.
for Biosensors as regardless whether Biosensors or Terumo creates the
sales channel into any clinical centre, Biosensors would be able to reap
the benefits. In fact, we think that the increased friendly competition of
these two companies for sales would work to push other competitors out
of these centres. Terumos recent revision of its licensing agreement with
Biosensors to lower revenue sharing but pay an upfront also indicates that
they are committed to pushing their NOBORI DES out strongly.
We think that this relationship will form a win-win situation
About relationships and revenue.
nature of its size and length of time in the market, would probably have a
wider marketing and relationship footprint than Biosensors. However, we
also note that Biosensors were the ones who initiated the trials in the EU
and have deep relationships with key opinion leaders in the field. During
the FY08 results update, management also indicated that there has been
a ramp up of experienced sales personnel that were previously from other
medical device companies. As such, we think that Biosensors will not be
too heavily disadvantaged in its direct sales efforts in the same EU playpen
as Terumo.
Xtent and Devax
US mid-cap medtech stocks take hit.
value adjustment in its 4
of warrants to purchase shares of a licensee (Xtent) as required by
accounting standards. This line item was non-cash in nature and is just a
reflection of the market value of Xtent.
Devax laying low.
investigator of the BioMatrix DES, is also the lead investigator for the Devax
AXXESS stent which caters to bifurcation conditions. Collectively, Devax
said in a pre-IPO filing that treatment of these bifurcation lesions results in
approximately 1m procedures per year. We recently interacted with Prof
Grube during the Singapore LIVE medical conference and gained positive
indications from him with regards to the Devax stent that utilises Biosensors
Biolimus A9 drug and its biodegradable polymer.
Leading cardiologist Eberhard Grube, who is the lead
What next for licensees?
facility, Biosensors will continue to work to fulfil its obligations but will now
only sell the Biolimus A9 drug to its licensees. Its licensees will now be
transferred the technology know-how for the formulation and coating of the
drug and biodegradable polymer for their respective stent platforms. This
resolves most operational issues of catering to the needs of its licensees.
In effecting the closure of the Newport Beach
JW Medical
Critical China piece.
Weigao remains a crucial piece in Biosensors revenue forecast of US$100-
115m for FY09 and US$250m in FY11. Discussions with management have
yielded positive feedback on the progress of the acquisition and we have
assumed the full acquisition of JWM by July 09.
The full acquisition of JW Medical from Shandong
Think win-win again.
this acquisition through. On one hand, Biosensors would gain an effective
entry into Chinas booming DES market through JWMs network and utility
of a low-cost manufacturing base. On the other hand, despite JWMs Excel
Stent continuing to draw good reviews and strong sales, we think that
incorporating Biosensors technology and know-how will better equip JWM
to compete against current market leaders Microport ang JNJ.
No questions on reputation.
shareholders, we are reassured that it continues to attract strong institutional
investors with Medtronic being the single largest shareholder. This helps to
reinforce our thesis that Biosensors and Shandong Weigaos management
will bring to the regulatory authorities a strong and credible case for the
JWM acquisition.
Taking a look at Shandong Weigaos
SFDA and Chinas priorities.
its second catastrophic natural disaster after the snow storm in early 2008
and is also in the midst of preparing for the Olympics. Although state
agencies continue to operate, we think that priorities are being diverted on
all fronts in order to prepare the entire country for a significant year of 2008.
As such, we think that some delays in processing the full acquisition
approval might occur in the run up to the Olympics. However, management
has continually emphasised that it will not be passively resting on its laurels
waiting for the approval from authorities. Although it did not give details,
CEO Michael Klein has indicated that he has alternative plans to push
ahead in China should the full acquisition of JWM prove too stumbling.
Evident from the news, China is now handling
Registration with SFDA.
requirement for foreign medical device companies. Roughly, it adds up to
about 82 working days for a new registration to run through the three offices
that are involved in the medical device registration process. However, it
may take up to double or triple that time for a successful registration due
to government inefficiencies. New regulations have also been implemented
by the SFDA to improve safety checks on drugs and medical devices that
may slow the process. However, our mention of Shandong Weigao and
Biosensors good reputation may work to help in the process.
Lower cost base.
Critical Care Products (CCP) Unit from Shandong Weigao on 8 May 08.
The slight delay caused a drop in gross margin for its CCP for FY08 but we
expect that the full porting over of manufacturing to eventually yield stronger
margins as it operates out of a lower cost base.
Section 5: Industry trends
Sustained investment interest in stents.
20 venture capital deals announced by companies developing stents or
stent-related products, totaling about US$320m. In Apr 08, two more deals
were announced with IDev Technologies raising US$25m and Tryton Medical
raising US$14m to further bring their stent technologies closer to market.
In Dec 07, REVA Medical raised US$42m from a bevy of high profile
investors, including Cerberus Capital and Medtronic.
Since 2003, there have been
Easing regulatory restrictions in UK.
agency that governs medical device usage in the UK, National Institute for
Health and Clinical Excellence (NICE), issued a statement on a possible
withdrawal on DES from its state health system due to the lack of data
supporting its benefits vs. its higher costs. However, in Feb 08, these fears
were alleviated when NICE issued a new statement endorsing the use of
DES as long as it is not more than £300 than a BMS. UK government data
has indicated that the average DES price is about £529 vs. £131 for BMS.
For Biosensors, we think that it will be able to offer a competitively priced
product to meet this requirement due to lower cost base of production in
Singapore.
Sometime back in Aug 07, the
Big boys problems.
competitors like Boston Scientific (BSX) and Johnson & Johnson (JnJ) are
positive for the company. As an overview, BSX continued its bottomline
compression due to its US$7b debt situation after its acquisition of Guidant
while JnJ is still at the back of the pack in terms of new innovations to fill its
DES pipeline after its Conor COSTAR DES stent failed to meet end goals
in May 07. Capitalising on its alliance with Terumo, we think Biosensors is
in a good niche position to acquire market share with its Biomatrix DES
platform.
Recent corporate reports on Biosensors main
Fertile grounds to boom.
DES space, especially with its recent CE mark inducing intense interest
from a clinical community that is pining for a safer next gen device. As can
be seen from VHAs Goodroe data, the utilisation of DES in stenting cases
seems to have started its turnaround in Dec 07 as more positive clinical
data presented highlighted the case for using DES vs. its low risk. Although
this is US data, we deem that the Rest of the World will mimic this trend
as the US continues to be a trendsetter in the medical device space.
Biosensors remains one of the only companies in this technology space
that operates in a low cost base along with fully owning the entire pipeline
of Intellectual Property ranging from its delivery system, to the biodegradable
polymer and proprietary drug Biolimus A9. Even BSX has to license its
Paclitaxel drug from another listed Canadian company, Angiotech.
Improving revenues from Big Boys.
and JNJ to obtain a gauge on the performance of their DES sales. As
indicated below, we see that both the companies are generally recording
improving QoQ revenue in various territories for their stent businesses. We
use their improving performances as the two largest stent manufacturers in
the world as a reflection of the better prospects for DES makers like
Biosensors with next-gen products.
Section 6: Risks
Bad clinical data.
data is low, we do not discount the possibility of it failing to meet
expectations. Should the LEADERS trial fail to meet clinician expectations
against J&Js Cypher stent, Biosensors earnings and share price might
be at risk.
Although the current likelihood of bad LEADERS trial
Aggressive price undercutting.
US$54m with an expected topline of US$100-115m in this financial year. In
the light of much bigger competitors like J&J (FY07 sales: US$61.1b, Cash:
US$7.8b) and Medtronic (FY07 sales: US$13.5b, Cash: US$1.1b) with a
stronger financial positions, aggressive price cuts to drive smaller companies
out of business could occur. Biosensors might not be able to meet
profitability guidance should a price war break out for a sustained period of
time.
Biosensors cash reserves are about
Overly intense competition.
entered into this space and technology innovation has been moving at a
breakneck speed. Should new or established cardiology companies put
out a better and safer technology into a stent, Biosensors might not be
able to compete effectively.
We acknowledge that many companies have
Bad execution.
in place to bring Biosensors into the next phase of growth, unforeseen bad
execution situations in China or Singapore manufacturing plants could be
its undoing. Slower than expected sales force infrastructure ramp up in its
many approved markets can also be a drag.
Section 7: Valuations and key drivers for Biosensors
Enough cash for 2 years.
agreement, Biosensors has settled for US$40m in upfront cash. Although
it will be recognised over a period of five years (about US$2m/quarter), the
full US$40m will be transferred to Biosensors at one go. With the current
US$54m in cash equivalents and an estimated burn rate of about US$40m/
year, we do not expect Biosensors to require any fund raising in the next
two years.
With the revision of the Terumo licensing
Turnaround story.
contribution from JWM, restructuring to cut redundancies, good
management in place and lower cost based productions in Singapore and
China, we urge investors to view their investment options in Biosensors
with a longer term horizon.
With a massive ramp up in BioMatrix sales, positive
Ruminating valuations.
strategic roadmap and has executed its plans well so far. Also, in a strong
show to ensure good operational execution, Biosensors CEO will now be
based out of Singapore. We use a standard medtech valuation methodology
by discounting its first year of substantial profit in FY10 to present day
value. Our fair value stands at S$1.04. Maintain
Appendix 1: Info on COURAGE trials
Confusion in the midst of COURAGE.
looked at 2,287 heart patients who suffer from chest pain (angina) but who
are otherwise considered low-risk for heart attack, and concluded that the
addition of stenting to optimal drug therapy resulted in no significant reduction
in heart attack or death. This set off a media firestorm of misinterpretation,
causing confusion for patients and physicians. We found a balanced
interpretation of the COURAGE trials and present it here in our report:
1.
The five-year COURAGE study,Can angioplasty and stenting save lives? In the case of a heart attack,
angioplasty definitely saves lives
COURAGE trial does not apply to patients who are having a heart attack;
2.
patients with advanced disease who are at risk for heart attack (Acute
Coronary Syndrome) angioplasty and stenting have been proven to be a
significant therapy for these patients;
3.
not revolutionary, but instead are consistent with current practice guidelines
from all major professional groups (AHA/ACC/SCAI) that recommend using
angioplasty and stenting only after medical therapy has proven inadequate;
4.
chronic stable angina are, in fact, at low risk for death or heart attack
stents in these patients are not intended to prevent death, but to relieve
pain and improve quality of life.
5.
still a proven treatment option for those whose quality of life (angina or
activity level) is not improved by medical therapy, or for those patients who
do not tolerate the side effects of medical therapy;
6.
did show that the scores for physical limitation, angina frequency, and
quality of life were significantly better for patients in the angioplasty group;
in fact,
angioplasty during the course of the trial because their angina was not
relieved by medication alone;
- many studies have proven this; theDo stents have proven value? COURAGE also does not apply toWill this trial change medical practice? The results of COURAGE areWere the patients in this trial at risk for heart attack? Patients withShould people with chronic stable angina get stents? Angioplasty isDo stents and angioplasty make people feel better? This initial report1/3 of the patients in the medications-only group switched over to
7.
to be as safe as medical therapy;
8.
chronic condition lifestyle changes, medications, stents are ways of
managing the disease and relieving symptoms, but they do not cure the
disease;
9.
Did all the patients in this study experience relief of chest pain?
No. In the COURAGE study neither therapy completely eliminated angina
for more than a quarter of the patients. This maybe due to the fact that the
COURAGE patients with stents had Bare Metal Stents (BMS) which may
have a higher rate of restenosis.
10.
Have patients with stable angina been given stents unnecessarily?
Under current practice guidelines, it is recommended that patients with stable
angina first be given a trial of medical therapy, along with lifestyle changes
and risk factor reduction. They are candidates for stents if they continue to
experience problems. What is unknown is how often these guidelines have
not been followed, and whether cardiologists have in fact recommended
stents as a first treatment option for this patient population. There is significant
controversy as to how often this occurs. Estimates of how many angioplasty
procedures are done in patients with stable coronary artery disease range
from 25% to 85%.
Appendix 2: Chinas healthcare trends
Booming trends.
device imports and exports in China actually exceeded US$10b for the first
time in history in 2006, with exports growing nearly 29% YoY. China could
have stated a total import/export medical device market of over $10b while
most industry reports value the Chinese medical device market at around
US$1 - 3b due to market division methodology.
Medtech Insight indicated that the total value of medical
2 parallel markets.
into two fairly parallel segments: high-end devices and low-end devices.
The high-end segment is dominated by a few large MNCs, while the lowend
includes a horde of about 3,600 domestic Chinese medical device
companies. In terms of market value, the high-end occupies only about
10% to 20% of the market while the other 80% to 90% is still predominantly
filled by cheap medical devices with minimal advanced technologies.
However, market growth is nearly twice as high in the high-end market
(about 20% YoY) compared to the low-end. As a result, it is usually the
low-end segment that is neglected when calculating the total market value.
The Chinese medical device market can be separated
Rising healthcare expenditure.
continues to grow in absolute terms although as a percentage, it hovers
around 4.5-5% of GDP. If China continues to spend about 4.7% of its GDP
for healthcare expenditure in 2006, we are seeing a CAGR (2000-2006) of
14% growth. This bodes well for Biosensors as it enters this market with
an established Chinese partner in JWM.
Chinas spending on healthcare
Are stents safe? In the COURAGE trial, angioplasty and stenting provedDo drugs or stents cure heart patients? Coronary artery disease is a
Management has shared in greater detail itsBUY
Although we are confident of the new executive team put
We compiled the data from BSX
We think that Biosensors is inch perfect in the
Biosensors recently completed its acquisition of the
We obtained a simplified workflow of registration
We feel that it is in both parties interest to push
Biosensors took a negative fairth quarter when it booked the decrease in fair value
We mentioned above that Terumo, by
We expect data from its 1700 patient trial, which is pitted
We note that Biosensors will still continue to
Management also gave a clear guidance
. Management has shared in greater detail itsBUY.
Fri Jun 13, 2008
J&J's Cordis president leaving company
CHICAGO, June 13 (Reuters) - Johnson & Johnson (JNJ.N: Quote, Profile, Research, Stock Buzz) on Friday said the worldwide president of its Cordis unit is leaving the company on July 11, the latest in a string of departures of senior executives from the vascular device maker.
No replacement has been named for Todd Pope, who had been with Cordis for less than two years.
Others departures include Company Group Chairman of Cordis Rick Anderson; Chief Medical Officer Dr. David Kandzari; vice president of sales Mark Valentine; the vice president of health economics, Brian Firth and his replacement, Liesl Cooper; and the vice president of clinical affairs, Denis Donohoe, who will leave this summer.
Cordis makes such devices as catheters and stents.
"Although expectations among investors for Cordis' stent franchise are low, we view these significant changes at Cordis as an underappreciated near-term risk for Cordis' business and a potential opportunity for its competitors, Abbott Laboratories (ABT.N: Quote, Profile, Research, Stock Buzz), Medtronic Inc (MDT.N: Quote, Profile, Research, Stock Buzz) and Boston Scientific Corp (BSX.N: Quote, Profile, Research, Stock Buzz) to capitalize on," said Wachovia analyst Larry Biegelsen said in a research note.
Biegelsen said he has heard that turnover in the sales force has also been high . A Cordis spokesman declined to comment.
*** The top executives head rolled. Sales staff left also because they all already know NEVO will never work and this Cordis ship is sinking like Titanic. Only the C.T.O and conman Conor CEO Frank Litvack is still around fanning smoke for the NEVO DES smoke screen.
Article date: 27/03/2008 on JNJ's RES-ELTION 1 clinical trial to be used for CE submission
A randomized clinical trial comparing the Conor Sirolimus-eluting Coronary Stent, a new cobalt chromium reservoir-base stent design, to the Taxus Liberte Paclitaxel-eluting Coronary Stent has begun according to Conor Medsystems, LLC and Cordis Corporation, the sponsors of the study.
"We are pleased that the RES-ELUTION trial has begun and that the first patient enrolled in this study occurred at our hospital. The product was easily delivered and performed well," said John Ormiston, M.D., North Shore Hospital, Auckland, New Zealand and Principal Investigator for this study. "The potential of sirolimus delivery from a fully-bioresorbable reservoir is exciting and may represent a breakthrough in the interventional treatment of patients with coronary artery disease."
The RES-ELUTION study is a randomized, multi-center comparison of the Conor Stent to the Taxus Liberte Stent in de Novo native coronary artery lesions. The primary endpoint of the study is angiographic in-stent late lumen loss at six months. The Conor Stent contains the same drug, sirolimus, as in the CYPHER® Sirolimus-eluting Coronary Stent, which is marketed by Cordis Corporation.
Secondary endpoints include target lesion failure, target vessel failure, major adverse cardiac events (MACE), stent thrombosis, target lesion revascularization, target vessel revascularization, and angiographic in-stent and in-segment binary restenosis at six months. Up to 50 patients will also be evaluated via intravascular ultrasound (IVUS) at six months.
The study will involve 388 patients at 40 sites worldwide including Australia, Belgium, Brazil, Denmark, France, Germany, New Zealand, The Netherlands and the United Kingdom. Patients will receive clinical follow-up at 30 days, six months and annually through five years.
Data from this trial will support a regulatory filing for a CE mark in countries outside the United States.
The unique Conor Medsystems technology is an important 'next generation' technology design that incorporates hundreds of small reservoirs, each acting as a depot into which drug-polymer compositions are loaded. This breakthrough design greatly enhances control of the rate and direction of drug delivery, enables a wider range of drug therapies, and potentially increases the range of clinical applications of drug-eluting stents and other drug-device combinations.
About Conor Medsystems, LLC
Conor Medsystems, LLC, a wholly-owned subsidiary of Johnson & Johnson, develops innovative controlled vascular drug delivery technologies, and has primarily focused on the development of drug-eluting stents to treat coronary artery disease.
About Cordis Corporation
Cordis Corporation, a Johnson & Johnson company, is a worldwide leader in the development and manufacture of interventional vascular technology. Through the company's innovation, research and development, Cordis partners with interventional cardiologists worldwide to treat millions of patients who suffer from vascular disease.
*** I expect 6 months later NEVO DES will flop like all the other Costar trials and JNJ got no more NEVO show left. LEADERS results will be out by then.
The time could be near...... end 2008 should be it
allright ( Date: 23-Jun-2008 15:56) Posted:
| Welcome Home. Okay I will listen to you guys and will be PATIENT..but at this rate may end up as a PATIENT....
|
|
Bollinger bands are really tight now. Large price change may occur.
The last time this happened, there was a upwards spike in price. However, at that time, the Acc/Dist chart was uptrending (a bullish sign).
But this time, there is no such signal.
Welcome Home. Okay I will listen to you guys and will be PATIENT..but at this rate may end up as a PATIENT....
I am back !!!! shit... yesterday landing at 6.20 am is the worst experience I have ever... it is raining, and thunder light can be seen every 10 seconds, but with our prestiguous SIA pilot, he is able to land perfectly... without any "twist and turns" on the runway... 2 thumbs up for SIA pilot....
Yupe the price can be disappointing, but from the 0.69 entry point of view, I think it has done a good job to sustain the price, you have to judge across the market performance.. I am pleased so far..
